_edited_edited_edite.png)

Lumbar Radiculopathy & Herniated Disc Treatment in Naples & Marco Island
If you have been told you have a herniated disc, a pinched nerve in the low back, or lumbar radiculopathy — or if leg pain following a clear pattern has come on after a back injury — this page is meant as a comprehensive resource. We walk through what is actually happening anatomically, why imaging findings often do not match the clinical picture, how the condition is properly diagnosed, and what modern treatment looks like at a pain practice that specializes in image-guided interventional care.
What lumbar radiculopathy actually is.
Lumbar radiculopathy is the medical term for symptoms caused by irritation or compression of a nerve root as it exits the lumbar spine. Each lumbar nerve root carries sensory and motor fibers to a specific region of the leg, so the symptoms — pain, numbness, tingling, weakness — follow a recognizable pattern based on which root is involved. When the cause is a herniated disc, the disc material has displaced beyond its normal boundary and is pressing on or chemically irritating the adjacent nerve root. Although patients (and many clinicians) use "herniated disc," "slipped disc," "pinched nerve," and "sciatica" somewhat interchangeably, these terms describe slightly different things. The disc herniation is the anatomic finding. Radiculopathy is the resulting nerve dysfunction. Sciatica is one specific pain pattern that results from irritation of the L5 or S1 nerve root and follows the sciatic nerve down the leg. A given patient often has all three.

OpenStax College, CC BY 3.0 <https://creativecommons.org/licenses/by/3.0>, via Wikimedia Commons
How a disc herniates.
Each intervertebral disc is built like a small biomechanical structure with three components: a tough outer ring (the annulus fibrosus), a gel-like center (the nucleus pulposus), and cartilaginous endplates that connect the disc to the vertebral bodies above and below. The annulus contains the nucleus under pressure and allows controlled motion of the spine. Over time, repetitive load, aging, and biomechanical strain cause the annulus to develop small tears. When a tear extends through the full thickness of the annulus, the nucleus can extrude into the spinal canal or the neural foramen. If that displaced disc material contacts or compresses a nerve root, the result is lumbar radiculopathy. Most lumbar disc herniations occur at L4–L5 or L5–S1, which together account for roughly 95 percent of cases. These are the segments that bear the most mechanical load and have the greatest range of motion in the lumbar spine.

Laboratoires Servier, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
How lumbar radiculopathy typically presents.

The hallmark feature is leg pain that follows a specific pattern, often described as deep, electric, or shock-like, and frequently radiating from the buttock down into the thigh, calf, foot, or toes depending on the nerve root involved. The pain is usually worse than the associated back pain — sometimes substantially so. Many patients describe the back as background ache and the leg as the dominant symptom. Specific patterns correspond to specific nerve roots. An L5 radiculopathy typically produces pain or numbness across the top of the foot, weakness lifting the big toe, and difficulty walking on the heel. An S1 radiculopathy typically produces pain down the back of the calf into the lateral foot and bottom of the foot, weakness with toe-off, and difficulty walking on tiptoes. An L4 radiculopathy is less common and produces pain down the front of the thigh into the inner calf, with weakness extending the knee. Symptoms are often worse with prolonged sitting, with bending forward, with coughing or sneezing (which raises intra-abdominal and intradiscal pressure), and during the first hour out of bed. Many patients find specific positions that ease the symptoms, often involving lying down with the hips and knees flexed.
Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436., CC BY 3.0 <https://creativecommons.org/licenses/by/3.0>, via Wikimedia Commons
Why "herniated disc on MRI" is not always the source of pain.
This is one of the most clinically important points in spine medicine. Disc herniations on MRI are extraordinarily common in adults who have no back or leg pain at all. Population studies have repeatedly shown that 30 to 40 percent of asymptomatic adults over 40 have a disc herniation on imaging, and the rate climbs with age. The imaging finding alone does not confirm the diagnosis. The diagnosis of clinically significant lumbar radiculopathy requires three things to line up: the patient's symptom pattern, the exam findings (sensory changes, reflex changes, weakness in the predicted distribution), and the imaging finding at the matching level. When all three correlate, the diagnosis is clear. When they do not, the workup looks further — at facet joint pain, sacroiliac dysfunction, peripheral nerve entrapment, or vascular causes — before attributing the symptoms to the imaging finding.

Davidjr74, CC0, via Wikimedia Commons
Red flags that need urgent evaluation.
A small number of lumbar radiculopathy presentations require urgent evaluation rather than routine outpatient care. These include progressive or rapidly worsening leg weakness, new bowel or bladder dysfunction, saddle anesthesia (numbness in the groin or inner thighs), and severe pain accompanied by fever or unexplained weight loss. The most concerning of these scenarios is cauda equina syndrome, which is a surgical emergency. Anyone with these features should be evaluated immediately rather than waiting for a routine appointment.
How lumbar radiculopathy is diagnosed.
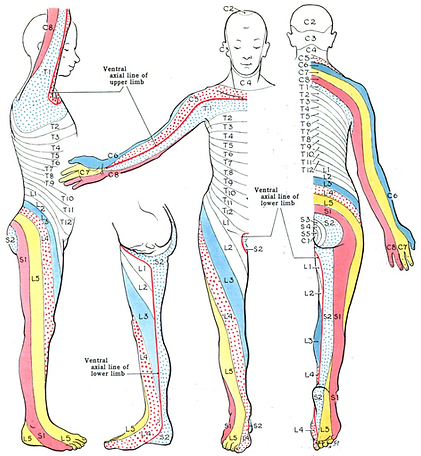
Diagnosis combines a focused history, a structured neurologic exam, and imaging — interpreted together rather than in isolation. The history establishes the timing, the trigger if any, the pattern of pain, what helps and what makes it worse, and the prior workup. The exam evaluates dermatomal sensation, deep tendon reflexes (the knee jerk for L4, the ankle jerk for S1), motor strength in specific muscle groups, and nerve tension signs such as the straight leg raise. MRI is the preferred imaging study when symptoms have not improved with initial conservative care, when red flags are present, or when interventional treatment is being planned. MRI shows the disc, the nerve roots, and the surrounding tissues in detail. CT is used in selected cases. Electrodiagnostic studies (EMG and nerve conduction studies) can confirm which nerve root is involved when the clinical picture is ambiguous, and can help distinguish radiculopathy from peripheral entrapment neuropathies.
Grant, John Charles Boileau, Public domain, via Wikimedia Commons
Treatment of lumbar radiculopathy.
Treatment is layered, with most patients improving substantially over weeks to months without surgery. The clinical reality, often underappreciated, is that the natural history of most disc herniations is favorable: the body reabsorbs disc material over time, inflammation around the nerve root settles, and symptoms gradually resolve. A well-designed treatment plan supports that natural process while controlling pain and preventing deconditioning.
Conservative care is the foundation. Targeted physical therapy emphasizes nerve-mobility techniques, core stabilization, postural mechanics, and a gradual return to function. Nerve-modulating medications — gabapentin, pregabalin, or low-dose tricyclics — can quiet neuropathic pain. Short courses of oral steroids are used selectively for severe acute presentations. Most patients with a fresh radiculopathy improve significantly with six to twelve weeks of structured conservative care.
Image-guided transforaminal epidural steroid injections are the cornerstone interventional treatment. Under fluoroscopic guidance, anti-inflammatory medication is delivered precisely to the affected nerve root, reducing inflammation at the source. For appropriately selected patients, transforaminal epidurals provide meaningful relief, accelerate recovery, and often avoid the need for surgery. Relief typically begins within a few days and may last weeks to months. Injections can be repeated as part of a long-term plan.
Selective nerve root blocks serve a dual purpose. They confirm which nerve root is driving the pain when the clinical and imaging picture is ambiguous, and they provide therapeutic relief at the same time. This is particularly useful when imaging shows changes at multiple levels and the question is which one matters.

Ahn K, Jhun HJ, Lim TK, Lee YS. Fluoroscopically guided transforaminal epidural dry needling for lumbar spinal stenosis using a specially designed needle. BMC Musculoskelet Disord. 2010 Aug 11;11:180. doi: 10.1186/1471-2474-11-180. PMID: 20698999; PMCID: PMC2927508.
Spinal cord stimulation is appropriate for selected patients with persistent radicular pain that has not responded to conservative care, injections, and where surgery is not desired or appropriate. Modern stimulation technology has substantially improved outcomes in well-selected patients.
Surgical decompression — microdiscectomy is the most common procedure — is appropriate when conservative and interventional care has not provided adequate relief, when neurologic deficit is progressing, or in cauda equina syndrome. Outcomes from microdiscectomy in well-selected patients are excellent. We coordinate with spine surgical colleagues when surgery is the right next step.
Treatment of central sensitization is layered in for patients who have lived with radicular pain for many months or years, since the nervous system component contributes meaningfully to ongoing symptoms once pain has been present that long.
Realistic expectations.
The good news for most patients with lumbar radiculopathy is that the natural history is favorable. The majority improve substantially with conservative care, with or without an epidural injection, over six to twelve weeks. A significant subset experience full resolution. A smaller subset have persistent symptoms that require longer-term interventional care, and a still-smaller subset benefit from surgical decompression. The trajectory is often non-linear — patients commonly experience a few good days followed by a setback, then more good days. This is normal recovery and does not signal that treatment is failing. The overall direction over weeks is what matters, not the day-to-day variation.
Patients who understand the favorable natural history, engage with structured conservative care, and use interventional treatment strategically tend to do substantially better than those who rush to surgery or who assume that imaging findings dictate their prognosis.
Our approach.
At Timeless Interventional of Naples, Dr. Chaturani Ranasinghe, MD, is a double board-certified anesthesiologist and interventional pain physician with extensive experience in image-guided spine procedures including diagnostic and therapeutic epidural injections, selective nerve root blocks, and the broader interventional approach to lumbar radiculopathy. We serve patients across Naples, Marco Island, and the broader Southwest Florida region, with coordination with spine surgical colleagues when appropriate.
When you're ready.
When you're ready, call to schedule a consultation or book online.
