_edited_edited_edite.png)

Spinal Stenosis Treatment in Naples & Marco Island
If you have been diagnosed with spinal stenosis — or if leg or arm symptoms that come on with standing, walking, or specific positions have been linked to spine narrowing on imaging — this page describes how we evaluate and treat the condition at Timeless Interventional of Naples, with focused interventional approaches for both lumbar and cervical stenosis.
What spinal stenosis actually is.
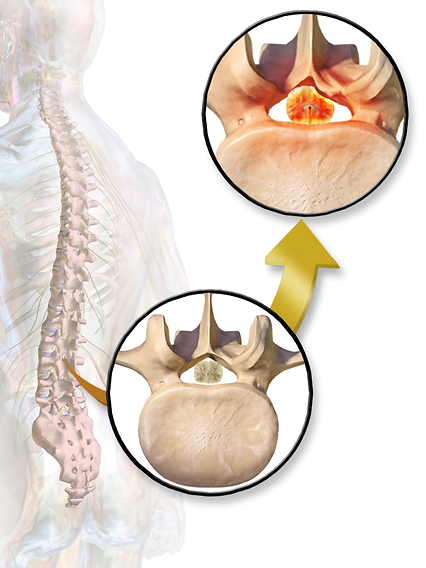
Spinal stenosis is narrowing of one or more spaces within the spine. The most clinically important spaces are the central canal (where the spinal cord and the cauda equina nerve bundle travel), the lateral recess (just to the side of the central canal, where individual nerve roots begin to exit), and the neural foramen (the opening through which each nerve root leaves the spine to travel to the body). Narrowing in any of these spaces can compress the nerves passing through, producing pain and neurologic symptoms.
Stenosis is typically the result of long-term degenerative change. As discs lose height, ligaments thicken (particularly the ligamentum flavum), and facet joints hypertrophy, the available space for nerves gradually decreases. It tends to develop slowly over years, which is part of why patients adapt around it for so long before seeking care.
Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436., CC BY 3.0 <https://creativecommons.org/licenses/by/3.0>, via Wikimedia Commons
Lumbar versus cervical stenosis.
Lumbar spinal stenosis is the most common form. It typically presents with neurogenic claudication — a pattern of leg pain, heaviness, numbness, or weakness that comes on with walking or standing, eases with sitting or forward bending, and is usually felt in both legs (though it can be asymmetric). The classic clue is that patients feel better leaning over a shopping cart or walking uphill, both of which flex the lumbar spine and open up the central canal.
Cervical spinal stenosis can produce arm symptoms (cervical radiculopathy) when the lateral recess or neural foramen is the primary site, or signs of spinal cord compression (cervical myelopathy) when the central canal is significantly narrowed. Myelopathic symptoms — hand clumsiness, gait imbalance, problems with fine motor tasks — are a more urgent finding and require careful evaluation.
How spinal stenosis is diagnosed.
Diagnosis is clinical and imaging-based. A detailed history identifies the characteristic positional pattern. An exam looks for neurologic signs, gait abnormalities, and patterns that point toward the involved level. MRI is the imaging modality of choice for evaluating the canal, lateral recess, and foramen at each level. In some cases, electrodiagnostic studies (EMG/NCS) can help distinguish stenosis from peripheral neuropathy or other nerve conditions.
Importantly, MRI findings of stenosis are common in asymptomatic adults over 60. As with facet hypertrophy, the imaging finding alone is not the diagnosis — the symptoms have to match the anatomy.

A. E. Francis, Public domain, via Wikimedia Commons
Modern treatment of spinal stenosis.
Treatment is layered, with the goal of restoring function and reducing pain without proceeding to surgery unless necessary.
Targeted physical therapy is foundational. Therapy for lumbar stenosis emphasizes flexion-biased exercises, core stabilization, and aerobic conditioning that respects the patient's positional limits. Cervical stenosis benefits from posture work, neck stabilization, and avoidance of provocative positions.
Image-guided epidural steroid injections are the cornerstone interventional treatment. The two main approaches are interlaminar epidurals (delivered between vertebrae into the epidural space) and transforaminal epidurals (delivered selectively to a specific nerve root). The choice depends on the involved level, the pattern of symptoms, and the anatomy. Relief typically lasts weeks to months and can be repeated as part of a long-term plan.
Nerve-modulating medications and addressing central sensitization play a supporting role, particularly for patients who have lived with stenosis for years.
Surgical decompression is appropriate when neurologic deficit is progressing or when interventional and conservative options have not provided adequate relief. We coordinate with spine surgical colleagues when surgery is the right next step.

-
Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. - Own work
Realistic expectations.
Spinal stenosis is rarely "cured" outside of decompression surgery, but it is highly manageable for many patients with a coordinated interventional approach. Realistic goals include longer comfortable walking distance, better sleep, reduced flares, and the ability to engage in activities that matter to you. Treatment is typically a series of refinements over months rather than a single procedure.
Our approach.
At Timeless Interventional of Naples, Dr. Chaturani Ranasinghe, MD, is a double board-certified anesthesiologist and interventional pain physician with extensive experience in image-guided lumbar and cervical procedures. We serve patients across Naples, Marco Island, and the broader Southwest Florida region, with coordination with spine surgical colleagues when appropriate.
When you're ready.
When you're ready, call to schedule a consultation or book online.
